While brainstorming and writing a proposal for a device to detect pediatric tuberculosis has been extremely valuable, we recognize the challenge of developing our devices as undergraduate/graduate students. This acknowledgement led us to try to identify a healthcare problem in Ghana and to come up with a solution that undergraduates could potentially pursue. The process began after we arrived in Ghana, with each student independently identifying a problem and brainstorming a solution. Next, we played an entrepreneurial game, in which each student gave a pitch for an idea, and everyone gave hypothetical money to his or her favorite idea. The ideas with the most hypothetical monetary investments would move on to the next round. After two rounds of pitches, we narrowed our list down to two ideas: Big Data and the Multi-Cot. Splitting up our group between the two ideas, we then prepared a presentation to give to Kumasi Center for Collaborative Research in Tropical Medicine (KCCR) researchers. Yesterday and today, we present the summaries of our ideas.
Kate Panzer (gave first-round pitch) ’18, Katharine Cocherl ’20, Kaila Helm ’20, Hope McMahon ’18
Throughout our time in Ghana, we had the opportunity to visit many hospitals and smaller health clinics. While visiting Komfo Anokye Teaching Hospital (KATH) in Kumasi, Ghana, we noticed that there was a poster on a pediatrician’s wall for the “One Baby One Cot” initiative. We soon learned that there is very limited space per patient at the large regional hospitals — certainly not enough space for each individual baby to occupy his or her own cot. For example, in some hospitals, there can be up to eight babies in one cot! This can be problematic when trying to prevent the spread of infection but also difficult for mothers who have little to no space to watch over their newborns when they stay at the hospital to breastfeed.
There are several implications of having multiple babies in a single cot that we would like to address. First, the risk of hospital-acquired infections greatly increases because of the close contact of the babies. This close contact also makes it difficult for nurses and caretakers to monitor each baby. In addition, many babies may need to be transported to other hospitals because of a lack of bed space, moving the patients and their caretakers farther from home.


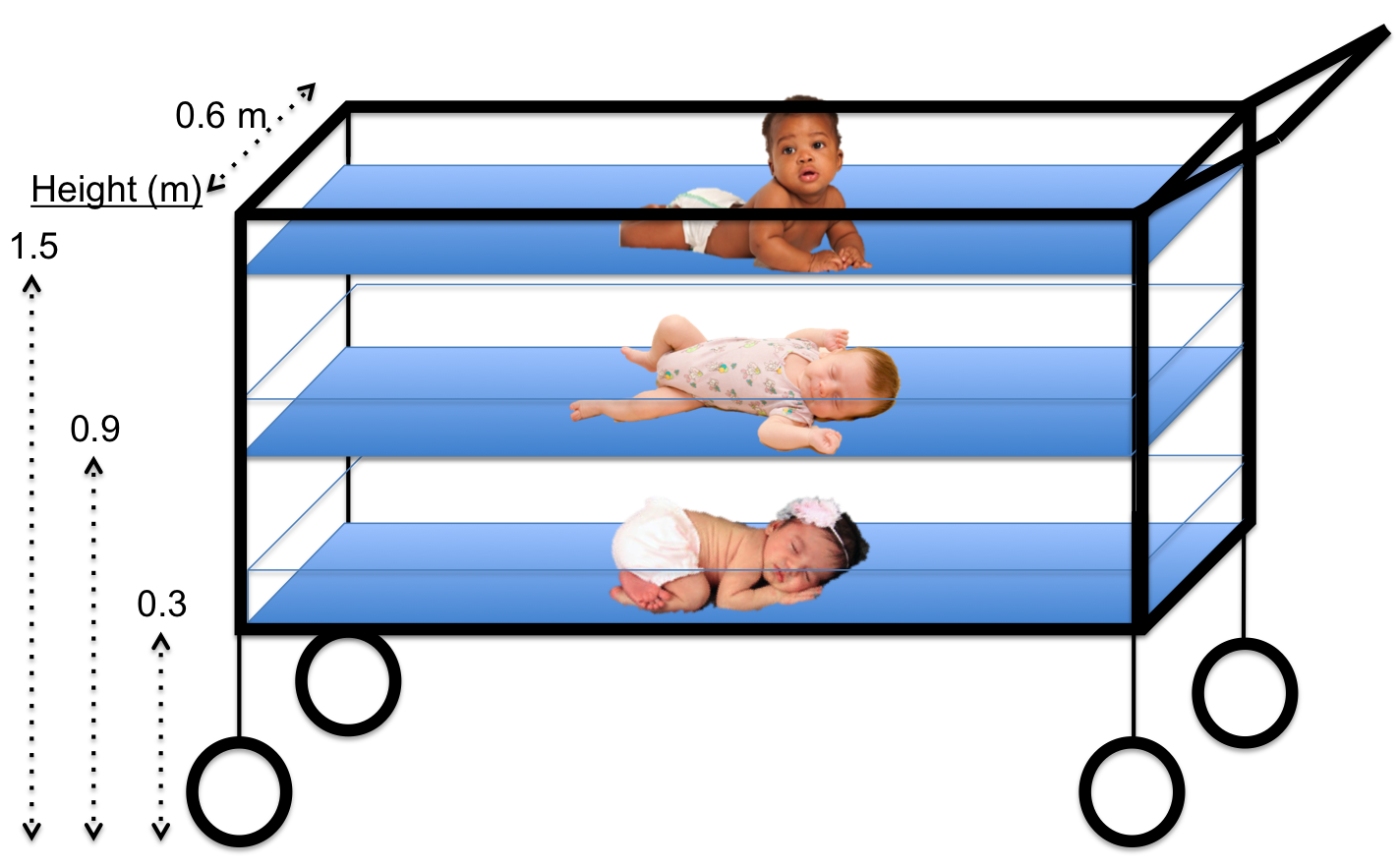
After learning about this problem, we began thinking of ways to decrease the complications associated with having multiple newborns in one cot. During the brainstorming session, the key element that led to our solution was actually how we view the problem. We started to see the issue as a lack of horizontal space – meaning the inability to add more cots horizontally without physically expanding the newborn ward. If expanding the horizontal space is not possible, then why not try to make better use of the vertical space that is already available? This concept of vertical space led us to the idea of the Multi-Cot, which involves three smaller newborn cots stacked vertically, with space between each cot to provide proper airflow. With clear plastic sides and an open top, each baby would be easily seen from every direction. Finally, to ensure safety when removing newborns from the lower levels, we added a sliding mechanism to our design to allow the lower cots to slide horizontally and eliminate any vertical obstructions when picking up the baby.
As we anticipate developing the Multi-Cot, we must consider multiple factors. Our main consideration is safety, which includes the Multi-Cot’s stability, the visibility of every child, and the ability to be sanitized. Other factors to be considered include the cost, as well as the ease of physical construction and dismantling; however, we would address these details later in the design process.