Here’s the promised interview with new faculty member Mike Mitchell, who starts as assistant professor of bioengineering at Penn in the Spring 2017 semester. Mike and editor Andrew E. Mathis discuss Mike’s background and education, where cancer research is now and where it’s heading, and just how big the radius is on the cheesesteak zone of impact around Philadelphia.
While brainstorming and writing a proposal for a device to detect pediatric tuberculosis has been extremely valuable, we recognize the challenge of developing our devices as undergraduate/graduate students. This acknowledgement led us to try to identify a healthcare problem in Ghana and to come up with a solution that undergraduates could potentially pursue. The process began after we arrived in Ghana, with each student independently identifying a problem and brainstorming a solution. Next, we played an entrepreneurial game, in which each student gave a pitch for an idea, and everyone gave hypothetical money to his or her favorite idea. The ideas with the most hypothetical monetary investments would move on to the next round. After two rounds of pitches, we narrowed our list down to two ideas: Big Data and the Multi-Cot. Splitting up our group between the two ideas, we then prepared a presentation to give to Kumasi Center for Collaborative Research in Tropical Medicine (KCCR) researchers. Yesterday and today, we present the summaries of our ideas.
The Multi-Cot aims to tackle the issue of limited space in large regional hospitals within Ghana and other similar situations of overcrowding.
Kate Panzer (gave first-round pitch) ’18, Katharine Cocherl ’20, Kaila Helm ’20, Hope McMahon ’18
Throughout our time in Ghana, we had the opportunity to visit many hospitals and smaller health clinics. While visiting Komfo Anokye Teaching Hospital (KATH) in Kumasi, Ghana, we noticed that there was a poster on a pediatrician’s wall for the “One Baby One Cot” initiative. We soon learned that there is very limited space per patient at the large regional hospitals — certainly not enough space for each individual baby to occupy his or her own cot. For example, in some hospitals, there can be up to eight babies in one cot! This can be problematic when trying to prevent the spread of infection but also difficult for mothers who have little to no space to watch over their newborns when they stay at the hospital to breastfeed.
There are several implications of having multiple babies in a single cot that we would like to address. First, the risk of hospital-acquired infections greatly increases because of the close contact of the babies. This close contact also makes it difficult for nurses and caretakers to monitor each baby. In addition, many babies may need to be transported to other hospitals because of a lack of bed space, moving the patients and their caretakers farther from home.
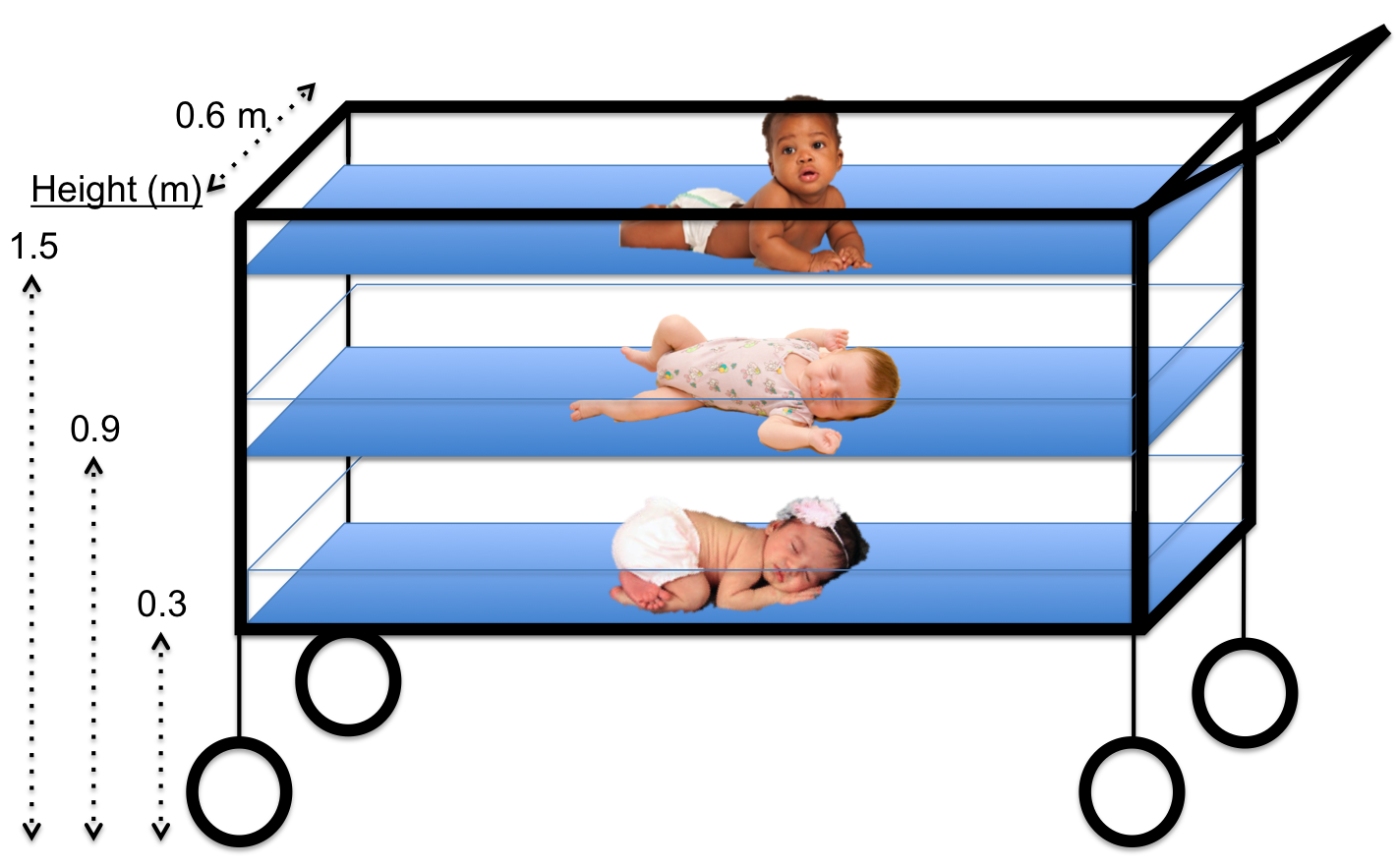
The horizontal sliding mechanism of the Multi-Cot allows each newborn to be safely removed from the structure, regardless of the cot level.
After learning about this problem, we began thinking of ways to decrease the complications associated with having multiple newborns in one cot. During the brainstorming session, the key element that led to our solution was actually how we view the problem. We started to see the issue as a lack of horizontal space – meaning the inability to add more cots horizontally without physically expanding the newborn ward. If expanding the horizontal space is not possible, then why not try to make better use of the vertical space that is already available? This concept of vertical space led us to the idea of the Multi-Cot, which involves three smaller newborn cots stacked vertically, with space between each cot to provide proper airflow. With clear plastic sides and an open top, each baby would be easily seen from every direction. Finally, to ensure safety when removing newborns from the lower levels, we added a sliding mechanism to our design to allow the lower cots to slide horizontally and eliminate any vertical obstructions when picking up the baby.
As we anticipate developing the Multi-Cot, we must consider multiple factors. Our main consideration is safety, which includes the Multi-Cot’s stability, the visibility of every child, and the ability to be sanitized. Other factors to be considered include the cost, as well as the ease of physical construction and dismantling; however, we would address these details later in the design process.
While brainstorming and writing a proposal for a device to detect pediatric tuberculosis has been extremely valuable, we recognize the challenge of developing our devices as undergraduate/graduate students. This acknowledgement led us to try to identify a healthcare problem in Ghana and to come up with a solution that undergraduates could potentially pursue. The process began after we arrived in Ghana, with each student independently identifying a problem and brainstorming a solution. Next, we played an entrepreneurial game, in which each student gave a pitch for an idea, and everyone gave hypothetical money to his or her favorite idea. The ideas with the most hypothetical monetary investments would move on to the next round. After two rounds of pitches, we narrowed our list down to two ideas: Big Data and the Multi-Cot. Splitting up our group between the two ideas, we then prepared a presentation to give to Kumasi Center for Collaborative Research in Tropical Medicine (KCCR) researchers. Today and Friday we present the summaries of our ideas.
Big Data: Deciphering Acoustic Trends in Tuberculosis, Pneumonia and Healthy Coughs
David Pontoriero (gave first-round pitch) ’18, Kathleen Givan ’20, Jason Grosz ’19, Danielle Tsougarakis ’20, Ethan Zhao ’19
Our goal was to think of a project that a team of undergraduates at Penn could complete in one year to produce something of value to KCCR in the scope of Ghanaian healthcare. We turned our attention toward big data science and the difficulties in tuberculosis diagnosis. One of the difficulties identified was the lack of diagnostic tools in more remote arms of the healthcare system. This lack leads to unnecessary and numerous referrals to larger care centers, inconveniencing the patient and placing a burden on the efficiency of the healthcare system.
Specifically, the only standard-of-care diagnostic ubiquitous throughout all clinics was patient-reported symptoms — the most notable of which is prolonged coughing. Moreover, this symptom can often be confused with asthma or pneumonia. However, asthma involves bronchial constriction, and TB and pneumonia have different sputum distribution profiles. We theorized that this difference would correlate with differentiated sound profiles for patient coughs or baseline breathing and, subsequently, measurable biomarkers. The idea proposed was that, if blind data could be collected from KCCR with sound recordings of patients coughing and breathing, along with their demographics and final diagnoses, then analyses could be run to produce an algorithm capable of differentiating between each cough or breath. This algorithm could then be extended to a phone app that could be used to more empirically diagnose patients in any setting and increase overall healthcare efficiency.
A “wiring diagram of the human brain,” produced using diffusion MRI scans of the brain.
A group of four scholars from the University of Pennsylvania, including Bioengineering professor Danielle Bassett, have issued a call in the journal Nature Human Behaviour for greater safeguards for patients as treatments in the field of neuroscience evolve and come ever closer to resembling “mind control.”
“While we don’t believe,” Bassett said, “that the science-fiction idea of mind control, totally overriding a person’s autonomy, will ever be possible, new brain-focused therapies are becoming more specific, targeted and effective at manipulating individuals’ mental states. As these techniques and technologies mature, we need systems in place to make sure they are applied such that they maximize beneficial effects and minimize unwanted side effects.”
I’m a rising junior studying Bioengineering at Penn. I’m also the founder of a music group called Band Dance Music (BDM). The overall premise of the group is to take the same music that a DJ plays at a college party but to play it with an 11-piece live band. The idea for this group started before I got to Penn, but it was something that I was confident in pursuing despite all of the other time commitments during the school year.
Starting a band at Penn was definitely a challenge. There are already so many music groups on Penn’s campus that it’s very easy for a group that is just starting out to get drowned out by other more prominent groups. After really pushing marketing hard for auditions, it actually was pretty easy to find students who were interested in the idea behind the group. Interestingly, of the 11 members that are now in the group, nine of them are actually in the School of Engineering and Applied Science.
While bioengineering and band dance music seem like two totally disparate fields, I was actually able to bridge the gap between these areas while taking ENGR105 with Professor Rizk. At the end of this course, we are asked to create a graphical user interface (GUI) that combines the entire course’s material. This GUI is completely free form – it can be in any area of interest that you like.
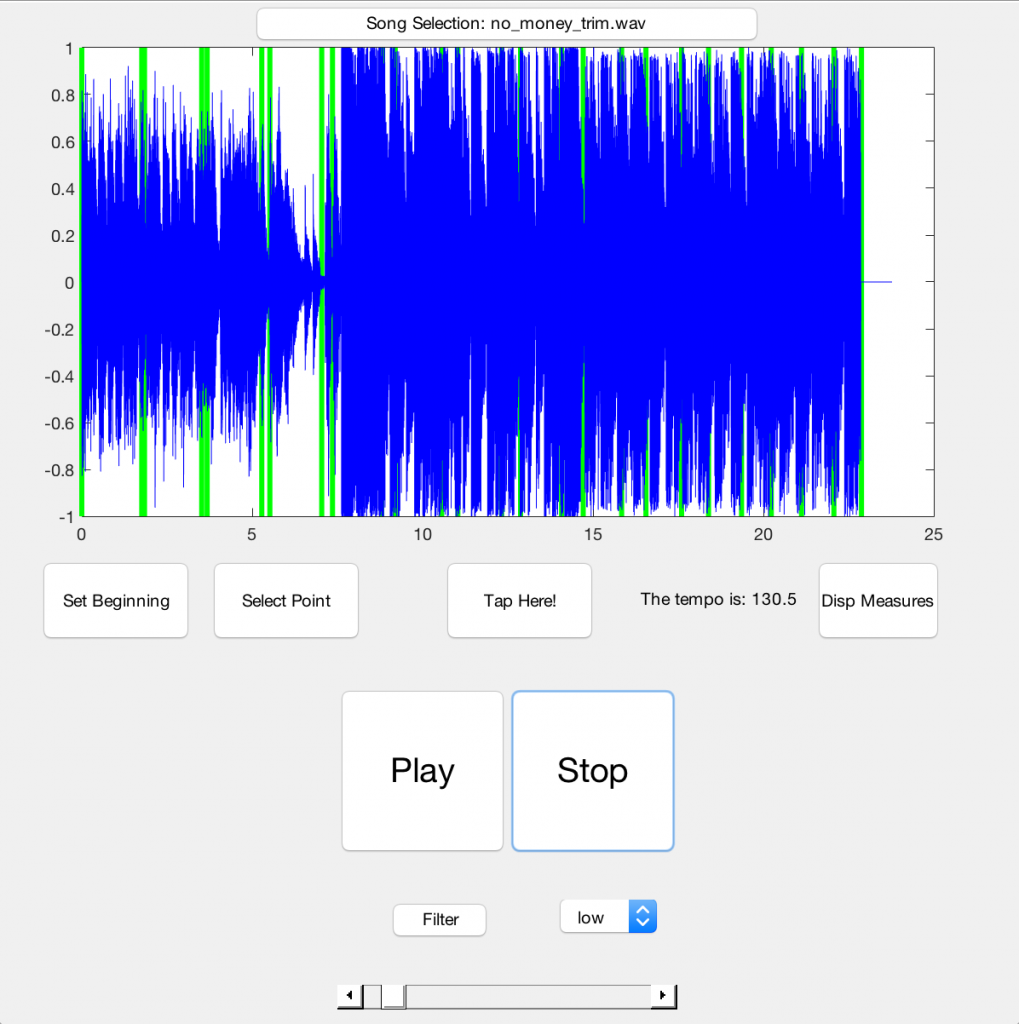
Since for a while I’d been having trouble arranging music completely by ear, I thought this would be the perfect opportunity to create a GUI that would help me arrange music for the band. There is rarely free time to spare during the school year, so being able to work on a passionate project of mine while also being able to complete my course work was a win-win situation. The GUI definitely took me longer than expected to create since it involved having to process electronic music into parts that would be easier to arrange, but I eventually was able to finish the interface. It featured a tap metronome, a filtering system, and a visual music player so I could streamline the music writing process. Below is a pictures of the GUI I created.
BDM is always looking for more interesting people to join who have a passion for this unique concept for a band. If any bioengineers reading out there are interested, feel free to reach out to me – I’d love to talk more about it. Thanks for reading!